

On June 2, 2026, the FDA released draft guidance that could reshape how gene therapies reach patients. The document, "Leveraging Prior Knowledge in the Developm...
Continue reading

Bipolar disorder has long been recognized as highly heritable, yet the biology underlying the condition has remained difficult to resolve. The genetics are comp...
Continue reading
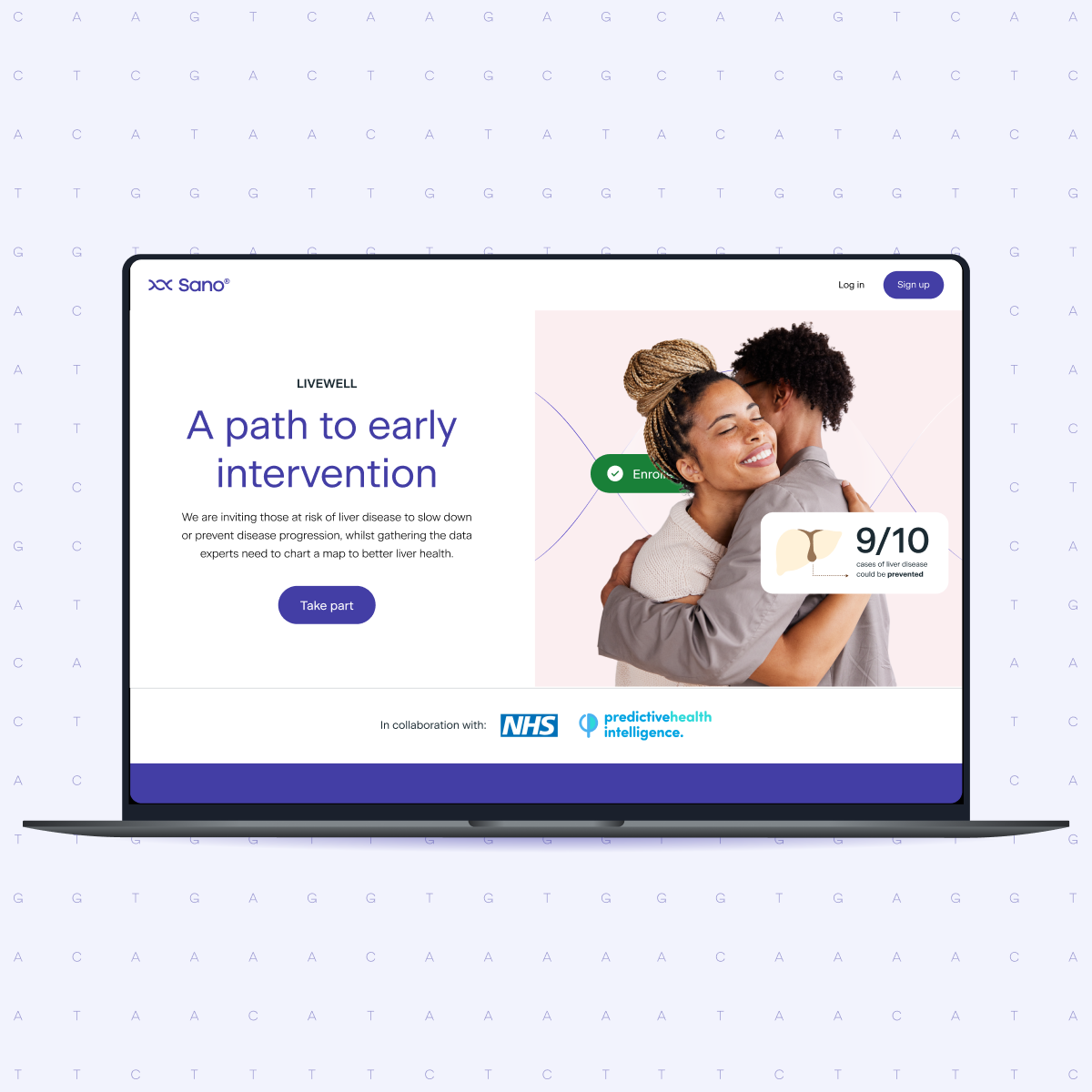
Finding patients who qualify for a clinical trial has always been one of the hardest parts of running one. In liver disease, particularly MASLD, it is especiall...
Continue reading

More than three decades after the Huntington's disease gene was cloned in 1993, there is still no approved therapy that alters the course of the disease. Recent...
Continue reading

When a clinical trial misses its enrollment targets, the instinct is often to look at recruitment through more channels, more outreach, and a bigger advertising...
Continue reading

In the most recent episode of The Genetics Podcast, host Patrick Short speaks with Dr. Paul Valdmanis, Associate Professor at the University of Washington, abou...
Continue reading
What four episodes of The Genetics Podcast reveal about the future of Alzheimer’s precision medicine
Alzheimer’s research is entering a new phase. For decades, the field has been shaped by the biology of amyloid plaques and tau tangles. Those remain central to ...
Continue reading

In the most recent episode of The Genetics Podcast, Patrick Short speaks with Dr. Sarah Marzi, Senior Lecturer at King’s College London and Group Leader at the ...
Continue reading

Precision medicine sponsors invest heavily to identify, educate, screen, consent, genotype, and support rare patients. In many programs, once a trial ends, that...
Continue reading

UK Biobank and similar resources have made an extraordinary contribution to biomedical research, enabling important advances across genomics, population health,...
Continue reading